In the ongoing debate about cholesterol and cardiovascular health—sparked by discussions around low-carb diets and elevated LDL in metabolically healthy individuals—Apolipoprotein B (ApoB) has emerged as a superior predictor of risk compared to traditional LDL cholesterol (LDL-C).
This post breaks down the key differences, backed by the latest evidence as of late 2025, and explains why focusing on ApoB provides a clearer picture of atherosclerotic risk.
The Fundamentals: What Do LDL-C and ApoB Actually Measure?
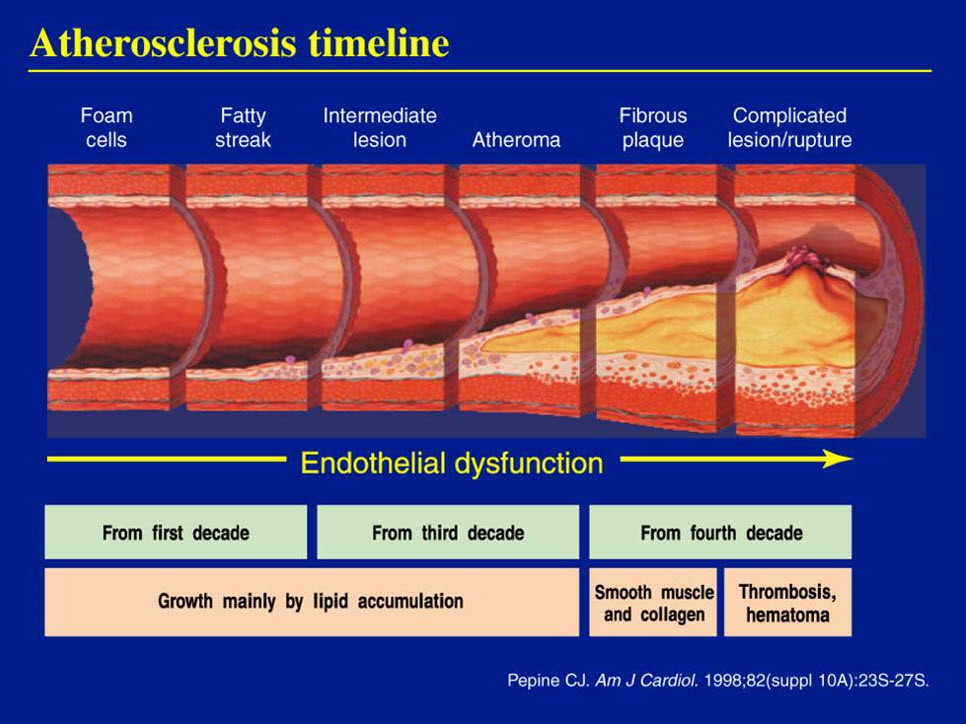
Atherosclerosis—the buildup of plaque in arteries—is driven by atherogenic lipoprotein particles entering and getting trapped in the arterial wall. These particles (primarily LDL, but also VLDL, IDL, and Lp(a)) each carry cholesterol, but it’s the number of particles that matters most for plaque formation.
- LDL-C: Measures the total cholesterol content within (mostly) LDL particles. It’s an indirect estimate and can vary based on how much cholesterol each particle carries (e.g., “fluffy” large particles vs. small dense ones).
- ApoB: Directly measures the total number of atherogenic particles, since there’s exactly one ApoB protein per particle (on LDL, VLDL, IDL, and Lp(a)).
When LDL-C and ApoB disagree (discordance)—common in conditions like insulin resistance, high triglycerides, obesity, or even low-carb diets—ApoB consistently predicts risk better.
The Evidence: ApoB Outperforms LDL-C
Recent meta-analyses and large studies in 2024–2025 reinforce ApoB’s superiority:
- A 2025 systematic review of 15 discordance studies (593,354 participants) concluded ApoB is the most accurate marker of cardiovascular risk, outperforming both LDL-C and non-HDL-C.
- UK Biobank data (2025) showed ApoB superior to LDL particle number (LDL-P) when discordant—even small mismatches (2%) with higher ApoB linked to elevated risk.
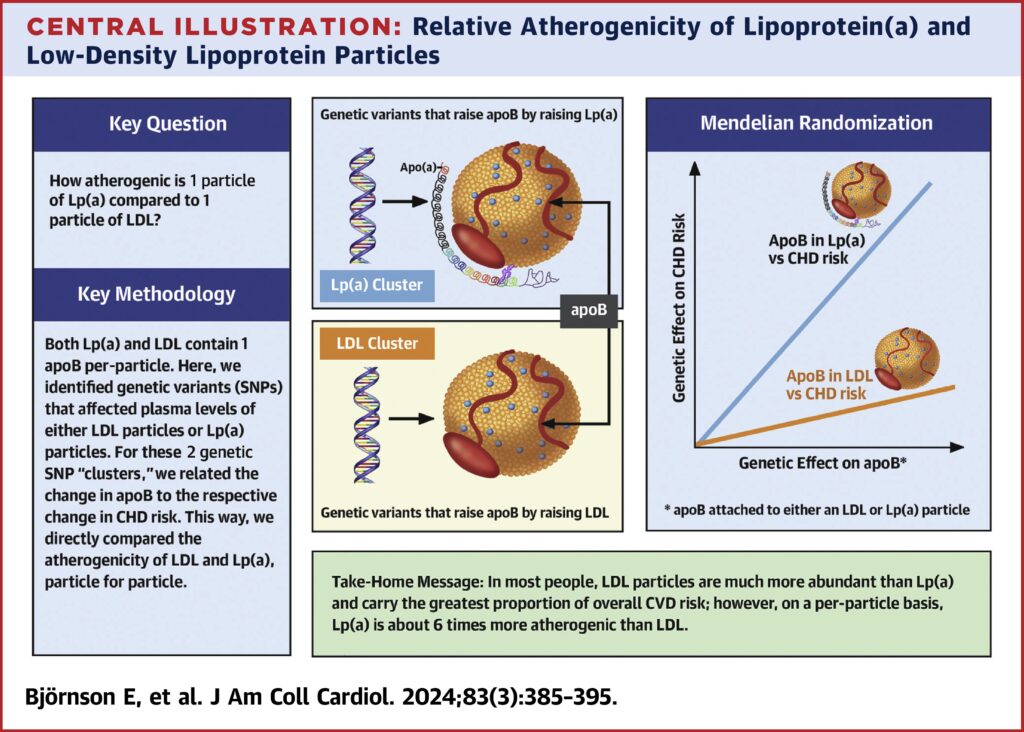
- Meta-analyses confirm ApoB as the strongest predictor in trials, observational data, and Mendelian randomization.
Guidelines reflect this shift:
- European Society of Cardiology (ESC/EAS): Recommends ApoB as preferred in high triglycerides, diabetes, obesity, or very low LDL-C.
- Canadian Cardiovascular Society: Longstanding preference for ApoB over LDL-C in certain cases.
- U.S. guidelines: Acknowledge ApoB as a risk enhancer, with growing calls for broader use.
Relevance to Low-Carb Diets and “Lean Mass Hyper-Responders” (LMHR)
Low-carb or ketogenic diets can dramatically raise LDL-C in lean, metabolically healthy people (the LMHR phenotype: high LDL-C, high HDL-C, low triglycerides).
- In LMHR, ApoB often rises alongside LDL-C.
- A 2025 KETO-CTA study (100 LMHR participants on long-term keto) found no rapid plaque progression over 1 year, with baseline plaque (not ApoB/LDL-C) predicting changes. However, this short-term pilot doesn’t prove long-term safety.
- Larger cohort data links low-carb high-fat diets to higher LDL-C, ApoB, and major adverse cardiovascular events (MACE), even after adjustments.
- No evidence yet exempts elevated ApoB from risk in LMHR—genetics, Mendelian randomization, and trials suggest it remains causal.
Bottom line: While low-carb diets offer metabolic benefits, elevated ApoB warrants monitoring. Advanced testing (e.g., ApoB, coronary calcium scan) can guide personalized decisions.
Key Takeaway
If you’re assessing heart disease risk—especially with diet changes or discordant lipids—prioritize ApoB. It’s a simple blood test that counts the actual culprits: atherogenic particles.
Ask your doctor for ApoB next time. Evidence as of 2025 strongly supports it as the gold standard over isolated LDL-C.
What are your thoughts on ApoB testing? Have you had it done? Share in the comments!
Leave a Reply
You must be logged in to post a comment.