
The PSA (prostate-specific antigen) test is a blood test used to help detect prostate problems, mainly prostate cancer, but also benign conditions like prostatitis (inflammation) and benign prostatic hyperplasia (BPH, enlarged prostate).
Here’s a breakdown of its validity:
✅ Strengths
- Simple & widely available – just a blood test.
- Can detect prostate cancer early – sometimes before symptoms appear.
- Useful for monitoring – helps track men already diagnosed with prostate cancer or on treatment.
⚠️ Limitations
- Not specific to cancer: PSA can be raised by infection, inflammation, recent ejaculation, cycling, or even medical procedures.
- False positives: High PSA does not always mean cancer, which can lead to unnecessary biopsies, anxiety, and treatment.
- False negatives: Some men with prostate cancer (especially aggressive forms) may have a normal PSA.
- Overdiagnosis: It often detects slow-growing cancers that may never cause harm in a man’s lifetime, but still lead to treatment and side effects.
🎯 Typical interpretation (very general guidance)
- < 3 ng/mL: Often considered within normal range for most men (age-adjusted cut-offs exist).
- 3–10 ng/mL: Grey area – further tests (repeat PSA, MRI, biopsy) may be needed.
- > 10 ng/mL: More likely to be associated with cancer, but not definitive.
🔍 Current medical stance
- The PSA test isn’t a perfect screening tool, but it is still widely used.
- In the UK, it’s offered through the NHS Prostate Cancer Risk Management Programme: men over 50 can request it, but it isn’t a national screening test because the benefits vs. risks are still debated.
- Doctors often use PSA alongside digital rectal examination (DRE), MRI scans, and sometimes genetic/family history assessments.
👉 Would you like me to summarise the latest UK recommendations (NHS & NICE) on when PSA testing is advised, and how it’s interpreted?
A “positive” PSA test (meaning a higher-than-expected result for your age) doesn’t automatically mean prostate cancer. The next steps usually follow a staged approach to rule out other causes first and only move toward invasive tests if needed.
Here’s what typically happens after a raised PSA result:
1.
Confirm the result
- Repeat the PSA test after a few weeks – sometimes levels are temporarily raised by infection, exercise, or even ejaculation.
- Your GP may check for urinary tract infection or prostatitis, and treat that before retesting.
2.
Assess individual risk
- Consider age, family history, ethnicity (e.g. Black men have higher risk), and previous PSA history.
- Sometimes a digital rectal examination (DRE) is done to feel for abnormalities.
3.
Further investigations if PSA remains high
- Multiparametric MRI scan (now standard in the UK) – can show whether there are suspicious areas in the prostate.
- If MRI is clear, you may just be monitored.
- If MRI shows something suspicious, the next step is usually a targeted biopsy.
4.
Biopsy (if needed)
- A biopsy takes small samples from the prostate to check for cancer cells.
- It carries risks (infection, bleeding, discomfort), so doctors try to avoid it unless clearly indicated.
5.
Follow-up pathways
- If cancer is found:
- Treatment depends on type/grade (Gleason score), stage, and your general health.
- Options: active surveillance, surgery, radiotherapy, hormone therapy.
- If no cancer is found:
- Ongoing PSA monitoring, sometimes repeat MRI if levels rise again.
- If result was due to benign causes:
- Treat underlying issue (e.g. prostatitis, enlarged prostate).
⚠️ Key point: A raised PSA is a starting signal for further assessment, not a diagnosis.
Would you like me to put together a step-by-step UK NHS pathway chart (from raised PSA → MRI → biopsy → treatment/monitoring), so you can see the decision flow clearly?
Here’s a clear UK-style pathway showing what typically happens after a raised PSA test result.
📊 Raised PSA Test – NHS Pathway
- Initial PSA Test Result
- PSA higher than expected for age.
- → GP checks history (age, family risk, ethnicity, symptoms).
- Confirm the Result
- Repeat PSA in ~4–6 weeks (rule out temporary rise).
- Check for infection (UTI, prostatitis).
- If infection found → treat, then repeat PSA.
- If PSA Still Raised
- Digital Rectal Examination (DRE).
- Refer to hospital (urology clinic) for specialist review.
- Hospital Tests
- Multiparametric MRI scan of prostate.
- Results:
- No suspicious area → may avoid biopsy, just monitor PSA.
- Suspicious area → targeted prostate biopsy.
- Biopsy (if done)
- Tissue samples examined under microscope.
- Results:
- Cancer found → treatment options discussed.
- No cancer → continue PSA monitoring, repeat MRI if needed.
- If Cancer is Diagnosed
- Team considers:
- Gleason score (aggressiveness).
- Cancer stage (localised vs spread).
- Overall health, life expectancy, patient preference.
- Options:
- Active surveillance (regular PSA & MRI, no immediate treatment).
- Surgery (prostatectomy).
- Radiotherapy.
- Hormone therapy or combinations.
- Team considers:
👉 In short: Raised PSA → repeat test → MRI → biopsy (if indicated) → treatment or monitoring.
Would you like me to turn this into a visual flowchart diagram so it’s easier to follow at a glance?
flowchart TD
A([Raised PSA test result])
B([Repeat PSA in 4–6 weeks\nCheck for infection])
C([PSA normal → Routine monitoring])
D([PSA still raised\n+/- DRE → Refer to urology])
E([Multiparametric MRI])
F([No suspicious area → Monitor PSA])
G([Suspicious area → Targeted biopsy])
H([Biopsy negative → Monitor PSA / repeat MRI])
I([Biopsy positive → Cancer diagnosis])
J([Treatment options:\nActive surveillance, Surgery,\nRadiotherapy, Hormone therapy])
A --> B
B -->|Normal / infection treated| C
B -->|Still raised| D
D --> E
E -->|Clear| F
E -->|Suspicious| G
G -->|No cancer| H
G -->|Cancer found| I
I --> J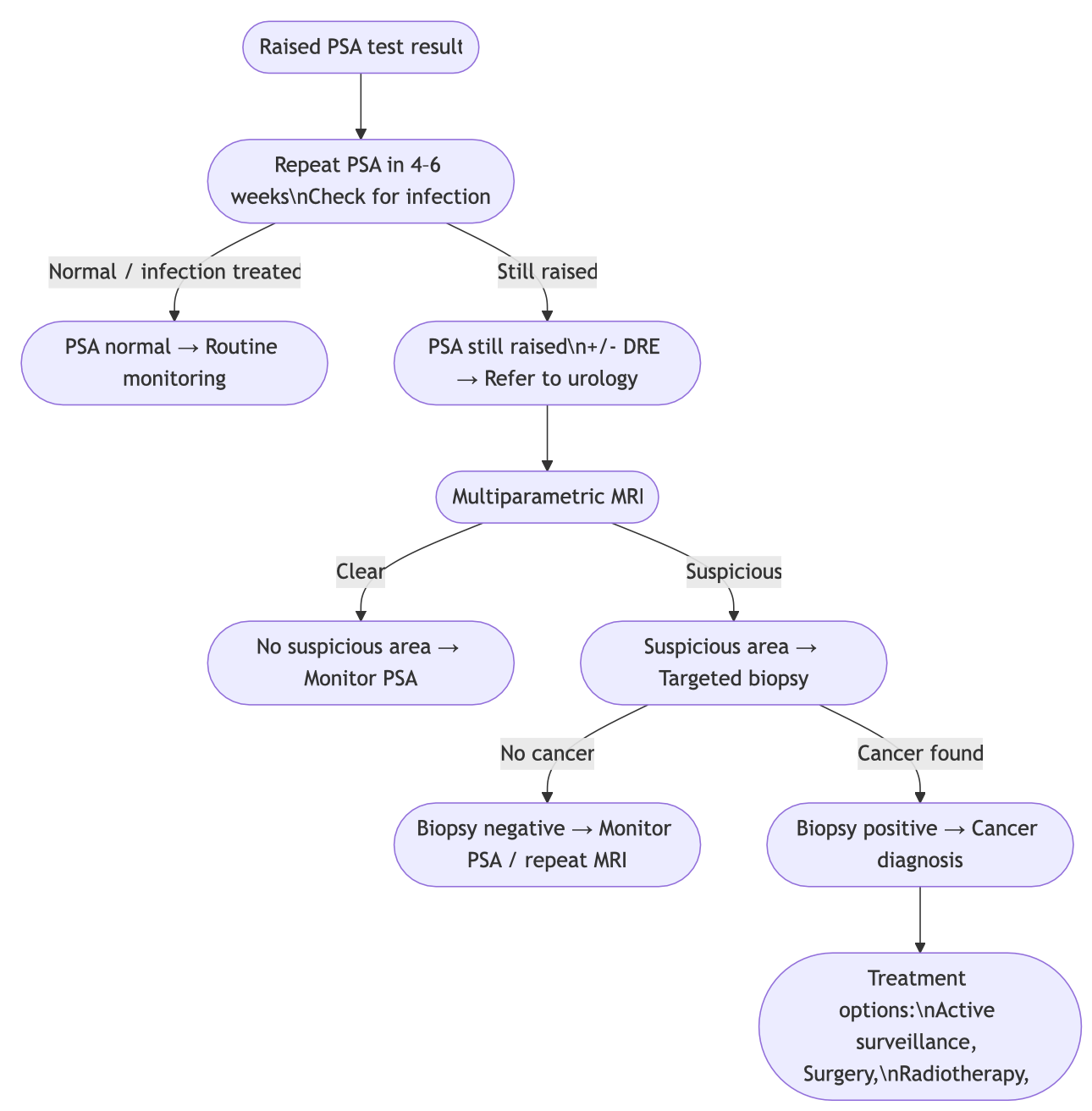
Leave a Reply
You must be logged in to post a comment.